Torticollis can occur at any age and may be congenital (present from birth) or acquired later in life. While many cases improve with early therapy, some require more targeted interventions depending on the underlying cause.
Symptoms of Torticollis
- Head tilted to one side with the chin rotated to the opposite direction
- Reduced range of motion in the neck
- Neck stiffness or discomfort
- Facial asymmetry or flattening of one side of the head (plagiocephaly)
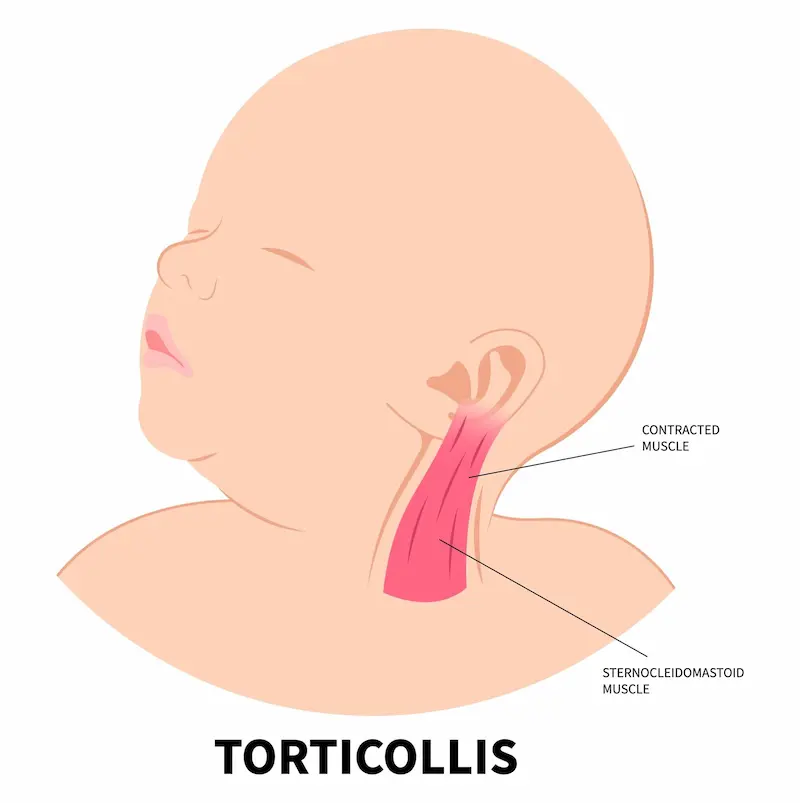
- A firm band or lump in the sternocleidomastoid muscle (common in infants)
- Feeding difficulties or delayed motor milestones in infants

Radiograph showing right‑sided head tilt…
Types of Torticollis
Congenital Torticollis
Congenital muscular torticollis has long been of clinical interest, not only in understanding its underlying mechanisms but also in determining the most effective treatment approach. A notable observation is that the characteristic sternocleidomastoid (SCM) mass is typically not present at birth and usually becomes apparent only after the first two weeks of life. This delayed appearance has led some authors to question whether all cases are truly congenital in origin.
Despite this, congenital muscular torticollis remains the most common form seen in infants. It is often associated with intrauterine positioning, birth trauma, or fibrosis of the SCM muscle. Early physiotherapy is highly effective, with most infants achieving full correction when treated promptly.
Acquired Torticollis
Develops later in life due to various causes, including:
- Atlantoaxial rotatory subluxation
- Neurological conditions such as dystonia or cerebral palsy
- Upper respiratory infections or inflammation
- Cervical spine abnormalities
- Infection or tumour
- Muscle spasm
- Visual or auditory issues leading to compensatory head posture
Management Options
Physiotherapy
The first‑line treatment, especially for infants. Includes stretching, positioning strategies, and motor development exercises. Most congenital cases improve significantly within the first year.
Manual Therapy
For older children and adults, manual therapy may help relieve muscle tightness and improve cervical alignment.
Traction
Skin or skeletal traction may be used in selected cases to restore neck alignment.
Botulinum Toxin Injections
Useful for spasmodic torticollis to relax overactive muscles and improve posture.
Surgical Intervention
Reserved for severe or persistent cases where conservative therapy is unsuccessful. Procedures may include SCM muscle release or lengthening, followed by rehabilitation.
Supportive Devices
- Soft neck collars for instability‑related cases
- Helmet therapy for infants with associated plagiocephaly
Conclusion
Torticollis is highly treatable when addressed early. A thorough assessment helps determine whether the cause is muscular, neurological, or structural — guiding the most effective treatment plan.
References
- Lee EH, Kang YK, Bose K. Surgical correction of muscular torticollis in the older child. Journal of Pediatric Orthopaedics. 1986;6(5):585‑589.
- Yu SW, Wang NH, Chin LS, Lo WH. Surgical correction of muscular torticollis in older children. Zhonghua Yi Xue Za Zhi (Taipei). 1995;55(2):168‑171. PMID: 7750058.