Spondylolysis (Pars Fracture) in Adolescents
Understanding a common cause of persistent back pain in young dancers and athletes, illustrated by a real clinical recovery journey
Spondylolysis is a stress fracture of the pars interarticularis — a small but important bony bridge at the back of the spine. It is one of the most frequent causes of persistent lower back pain in adolescents, particularly those involved in sports or activities that require repetitive spinal extension.
When identified early, spondylolysis is often managed successfully. When diagnosis is delayed, symptoms may persist and, in some cases, progress to spinal instability. This article provides a clinically guided overview together with a real patient story to help families better understand the condition and its management.
A Ballet Dancer’s Story

At just 14 years of age, she was training at an advanced level in ballet, attending regular classes and rehearsals that demanded discipline, precision, and repeated lumbar extension. Over time, she developed a dull, persistent ache in her lower back. There was no single fall or dramatic injury — just pain that slowly became part of everyday training.
Like many young dancers, she initially believed the discomfort was simply part of rigorous practice. However, when the pain persisted despite rest and began to affect sleep and performance, her family sought specialist assessment.
A comprehensive clinical evaluation and advanced imaging confirmed bilateral spondylolysis at the L5 level. The findings were consistent with a stress fracture that had developed gradually from repetitive extension and axial loading.

A structured period of non‑operative management was undertaken, including activity modification and rehabilitation. Despite this, her pain persisted and continued to limit training. After careful discussion with the family, a shared decision was made to proceed with direct pars repair, a motion‑preserving surgical technique designed to stabilise the fracture while maintaining spinal mobility.


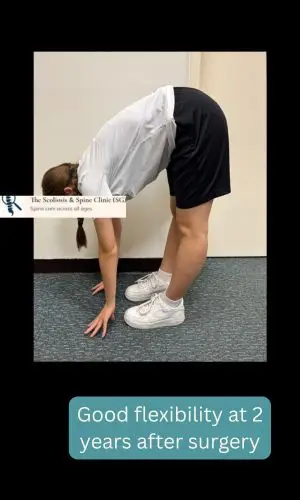
Her recovery progressed smoothly with graduated rehabilitation. At two‑year follow‑up, she reported being pain‑free in day‑to‑day activities and during dance training. Clinical examination demonstrated good functional recovery, with the ability to bend forward and extend the lumbar spine without discomfort.
She has since returned to full ballet performance. Her experience highlights that, when accurately diagnosed and appropriately managed, adolescent spondylolysis can be treated while preserving spinal motion and long‑term function.
Her Recovery Journey – Returning to Ballet Two Years After Surgery
Other Possible Causes of Back Pain in Adolescents
- Muscle strain and overuse injuries
- Intervertebral disc pathology (slipped disc)
- Apophyseal stress injuries (apophyseal ring fracture)
- Sacroiliac joint dysfunction
- Postural or biomechanical imbalance
Management
Conservative Treatment
- Activity modification
- Physiotherapy focused on core control and biomechanics
- Bracing in carefully selected cases
Surgical Treatment
Surgery may be considered in appropriately selected adolescents when symptoms persist despite structured conservative care or when spinal stability is compromised. Motion‑preserving techniques such as direct pars repair may be suitable in selected cases.
Frequently Asked Questions
Who should assess a child or adolescent with suspected spondylolysis?
One of the most common challenges in managing spondylolysis is delayed or incomplete diagnosis. Assessment by an orthopaedic surgeon with a special interest in spinal biomechanics is important to establish an accurate diagnosis, assess fracture stability, and guide appropriate treatment.
The role of the spine surgeon is to clarify the underlying cause of pain and reduce the risk of the condition progressing into a chronic non‑union. Other specialties, such as sports medicine or pain management, may focus on symptom control but have different clinical priorities.
Is surgery required for most patients with spondylolysis?
No. The majority of adolescents with spondylolysis do not require surgery. With early diagnosis and appropriate management — including activity modification, physiotherapy, and time — many patients experience good symptom resolution.
How long is the recovery period?
Recovery time varies depending on the stage of the fracture and individual response to treatment. In many cases, improvement is seen over a period of six weeks to three months.
During recovery, serial imaging, including follow‑up X‑rays where appropriate, can be helpful in monitoring fracture healing and spinal stability.
When is surgery considered?
Surgery may be considered when pain persists beyond approximately three months despite structured conservative treatment, particularly when imaging demonstrates that the fracture has progressed to a non‑union.
In selected patients, motion‑preserving surgical options such as direct pars repair may be considered to stabilise the fracture while maintaining spinal mobility.
Disclaimer: This article provides general medical information and is not a substitute for personalised assessment. Individual conditions vary. Please seek professional medical advice for diagnosis and treatment.