Pain Management From a Spine Doctor’s View: Understanding Diagnosis, Procedures, and Treatment Options
Dr Lau provides a comprehensive spine-focused pain management service that begins with accurate diagnosis.
Many patients experience pain from nerves, discs, joints, or stress injuries — and the right treatment depends on identifying the true source.
This guide explains how spine doctors assess pain, when pain procedures are considered, and how these options fit into a safe, structured treatment plan.
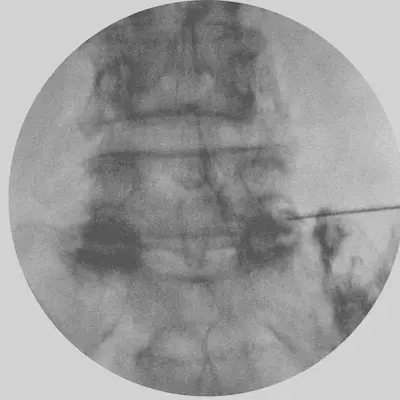
L5–S1 Radiofrequency Stimulation to the Dorsal Root Ganglion
Quick Summary
Pain procedures can serve two roles: diagnostic and therapeutic.
Diagnostic procedures help identify the exact source of pain by temporarily numbing a specific structure.
Therapeutic procedures aim to reduce inflammation or suppress pain when the underlying problem cannot be fully reversed.
The table below shows how spine doctors decide when to relieve pain, when to suppress pain, and where pain procedures may be considered.
The highlighted column shows where pain procedures may be considered in each situation.
Situation
What’s happening
What we do
Where pain procedures fit
Problem will get better
The spine is healing
Pain relief
Sometimes used
Problem cannot be fixed
Permanent changes
Pain suppression
Main option
Problem can be fixed with surgery
Correctable cause
Treat the cause
Not the main treatment
Pain without clear cause
Many small factors
Pain procedures + rehab
Used to control symptoms
Why You Should First See an Orthopaedic Surgeon With a Spine Interest
Pain procedures should never be the first step. The first step is always a proper diagnosis. A spine-trained orthopaedic surgeon can:
Identify whether the pain comes from a nerve, disc, joint, bone, or muscle
Check if the problem is reversible, permanent, or surgically correctable
Ensure no serious condition is missed
Guide you to the safest and most effective treatment
Some spine surgeons — including Dr Lau — also perform pain procedures.
This means diagnosis and treatment come from someone who understands the entire spine pathway.
Objective 1 — Relieve Pain While the Body Heals
Many spine problems improve naturally. Pain relief helps patients stay active while the body recovers.
Bracing — for example, in cases with stress fractures or pars defects
Objective 2 — Suppress Pain When the Problem Cannot Be Fixed
Some spine problems cannot be reversed. In these cases, the goal is long-term pain control and improved function.
Procedures Used in Spine Pain Management
A. Procedures That Help Identify the Pain Source
Selective Nerve Root Block (SNRB) — numbs one nerve to confirm the level
Facet Joint Block — checks if the facet joint is the pain source
Medial Branch Block — confirms facet pain before RFA
Sacroiliac Joint Block — identifies SIJ pain
Discography — rarely used today
Pars Defect Diagnostic Block — helps confirm pain from a pars fracture (spondylolysis)
Clinical Note: Pars Defect Diagnostic Block
Pars defects — also known as
spondylolysis
— are stress fractures that can mimic disc or facet pain.
A targeted diagnostic block helps confirm whether the pars defect is the true pain generator.
Dorsal root ganglion (DRG) stimulation(See the photo above)
Intrathecal pain pumps
C. Disc Pain Procedures (Biacuplasty & Nucleoplasty)
1. Biacuplasty (Disc Pain Treatment)
Biacuplasty uses two cooled radiofrequency probes inside the disc to reduce disc pain.
It is useful for discogenic pain, especially when Modic changes are present.
2. Nucleoplasty (Percutaneous Disc Decompression)
Nucleoplasty is a minimally invasive procedure that removes a small amount of disc material to reduce pressure inside the disc.
It is considered for contained disc protrusions that cause persistent back or leg pain despite conservative treatment.
D. Procedures That Do Both (Diagnose + Treat)
Procedure
Identify?
Treat?
Notes
Selective nerve root block
✔️
✔️
Confirms level + short relief
Facet joint injection
✔️
✔️
Confirms + treats
SI joint injection
✔️
✔️
Confirms + treats
Medial branch block
✔️
❌
Diagnostic before RFA
Biacuplasty
✔️ (selected)
✔️
Disc pain diagnosis + treatment
Nucleoplasty
✔️ (indirect)
✔️
Reduces disc pressure; useful for contained protrusions
Frequently Asked Questions (FAQ)
1. When does a pain specialist come into the picture?
You should first see an orthopaedic surgeon with a spine interest. They will make the diagnosis, determine the underlying cause, and outline the treatment plan.
If the problem does not improve with appropriate treatment, a pain procedure or surgery may be suggested depending on the objective — whether the goal is to relieve pain while the body heals, suppress pain when the problem cannot be fixed, or treat the cause directly. When the pain procedure is required, pain specialists may come into picture. Pain specialists may also help to adjust pain medications to minimize side effects.
2. Why do I need a pain procedure after surgery?
Surgery may not always achieve its full objective. This can be due to anatomical constraints, the severity of the condition, or the patient’s overall health.
In such cases, pain suppression may still be necessary after surgery to improve comfort and function. Pain procedures help manage residual symptoms when further surgical correction is not appropriate or not possible.
3. Who can perform pain procedures?
Pain procedures should only be performed by a qualified clinician who is properly trained in this area.
These procedures are commonly performed by orthopaedic surgeons with an interest in spine surgery or by pain specialists.
Both groups are trained to understand the underlying diagnosis, select the appropriate procedure, and perform it safely.
4. What is radiofrequency?
Radiofrequency (RF) refers to controlled heat energy delivered through a specialised needle.
It is used to reduce pain signals from specific nerves, especially those supplying the facet joints or the dorsal root ganglion (DRG).
5. How does radiofrequency ablation work?
Radiofrequency ablation works by applying heat to a targeted nerve to interrupt its ability to send pain signals.
The procedure does not damage the surrounding structures and is performed under imaging guidance for accuracy.
Pain relief can last months to years, depending on the condition and the nerve involved.
6. What is the DRG (Dorsal Root Ganglion)?
The dorsal root ganglion (DRG) is a small nerve structure located just outside the spine.
It acts like a “relay station” that processes pain signals before they travel to the spinal cord and brain.
When irritated or compressed, the DRG can cause severe nerve pain — and targeted procedures such as DRG blocks or DRG radiofrequency can help reduce these symptoms.
7. Why does chronic pain become difficult to treat?
Chronic pain becomes difficult to treat when the nervous system becomes sensitised over time.
Even after the original injury improves, the nerves may continue sending amplified pain signals.
Factors such as prolonged inflammation, nerve irritation, stress, and reduced movement can all contribute.
Early diagnosis and appropriate treatment help prevent this progression.