Coccydynia commonly presents as pain when sitting, leaning backward, or rising from a chair. This article explains how tailbone pain presents, what causes it, and how it is typically managed in Singapore. Occasionally, patients may report that the pain originates slightly higher, over the lower sacrum — particularly around the S4 or S5 region — rather than the coccyx itself.
What Is Coccydynia?
Coccydynia refers to pain originating from the coccyx, the small triangular bone at the lower end of the spine. Pain is often worse when sitting on hard surfaces, leaning backward, or transitioning from sitting to standing. Some patients may experience mild radiation into the buttock region.
What Are the Symptoms?
- Sharp or aching pain at the tailbone region
- Pain when sitting, especially on hard or narrow surfaces
- Discomfort when leaning backward or slouching
- Pain when moving from sitting to standing
- Localised tenderness over the coccyx
- Pain during bowel movements (in more severe cases)
- Occasionally, pain during sexual intercourse
What Causes Coccydynia?
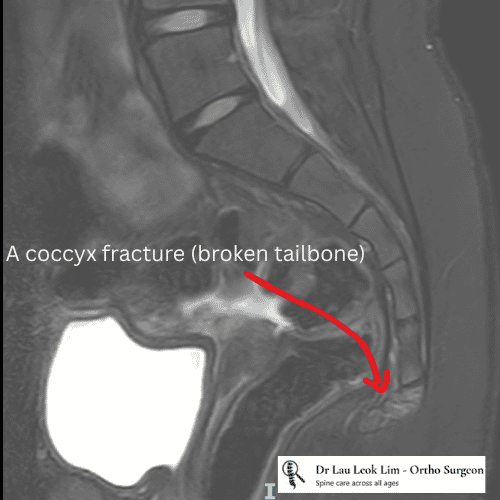
- Direct trauma from a fall onto the buttocks — the most common cause seen in clinical practice
- Sports injuries or repetitive impact to the coccyx
- Prolonged sitting on hard surfaces, especially in thinner individuals with less natural padding
- Pregnancy or childbirth‑related strain
- Idiopathic causes (no clear trigger identified)
How Is Coccydynia Diagnosed?
- Clinical examination of the coccyx and pelvis
- Palpation to assess tenderness and mobility
- X-ray to evaluate alignment, fractures, or deformity
- MRI when soft tissue inflammation or other pathology is suspected
- Diagnostic injections to confirm the coccyx as the pain source
What Are the Treatment Options?
Non-Surgical Management
- Activity modification and avoiding prolonged sitting
- Use of coccyx cushions (donut or wedge)
- Posture correction and ergonomic adjustments
- Physiotherapy for pelvic floor and core stability
- Oral anti-inflammatory medications
- Manual therapy or mobilisation
Interventional Procedures
- Coccygeal steroid injections
- Ganglion impar block for chronic or severe cases
Surgical Management
- Coccygectomy (removal of the coccyx) — reserved for rare, severe cases
- Considered only after failure of comprehensive non-surgical treatment
When Should You See a Spine Specialist?
- Pain persisting for more than 6–8 weeks
- Difficulty sitting for work, travel, or daily activities
- Pain affecting sleep or mobility
- Tailbone pain after a fall
- Symptoms worsening over time or associated with red flags
Conclusion
Coccydynia can be painful and disruptive, but many cases improve with structured, stepwise management. Early evaluation helps rule out other causes, guide targeted therapy, and support a safe return to comfortable sitting and daily activities.
References
- Fogel GR, Cunningham PY III, Esses SI. Coccygodynia: Evaluation and Management. Journal of the American Academy of Orthopaedic Surgeons. 2004;12(1):49‑54.
FAQ
1. Is coccydynia always caused by a fall?
No. Falls are common triggers, but prolonged sitting, degenerative changes, childbirth, or idiopathic causes are also possible.
2. How long does coccydynia take to improve?
Many patients improve over weeks to months with cushions, posture correction, and therapy.
3. Do I always need an MRI?
Not always. MRI is used when symptoms are atypical or severe.
4. Are injections safe?
Yes — when performed by experienced clinicians under imaging guidance.
5. Will I need surgery?
Surgery is rarely required and reserved for severe, persistent cases.
6. Do cushions help?
Yes. Coccyx cushions reduce pressure and improve sitting tolerance.
7. Can posture or work setup contribute?
Poor ergonomics can aggravate tailbone pain.