What Is Anterior Cervical Spine Surgery?
Anterior cervical spine surgery is performed through a small incision at the front part of the neck to relieve pressure on the spinal cord or nerve roots. This approach is muscle‑sparing and provides direct access to the cervical discs.
Anterior approach — performed from the front part of the neck.
Why Is Surgery Needed?
Surgery is considered when symptoms persist despite non‑surgical treatment, or when MRI shows significant nerve or spinal cord compression. Common reasons include arm pain, numbness, weakness, or signs of cervical myelopathy such as imbalance or hand clumsiness.
Related conditions: Cervical Radiculopathy | Cervical Myelopathy
The Surgical Objective
The primary goal of anterior cervical surgery is to decompress the nerve or spinal cord and restore a safe, stable environment for the cervical spine. This objective always comes before choosing the approach or technique.
ACDF — Anterior Cervical Discectomy and Fusion
ACDF removes the damaged disc, decompresses the nerve or spinal cord, and stabilises the spine using a cage and small plate. It is a reliable, time‑tested procedure suitable for severe degeneration, multi‑level disease, or instability.
Surgical Dose
A single‑level ACDF is considered a minimal surgical dose. Because the anterior approach is muscle‑sparing, recovery often follows a pathway similar to minimally invasive surgery.
ADR — Artificial Disc Replacement
ADR replaces the damaged disc with a mobile artificial disc to preserve natural neck motion. It is ideal for younger patients with soft disc herniation and healthy facet joints. It may not be suitable for advanced degeneration, instability, or osteoporosis.
ACDF vs ADR — Visual Comparison
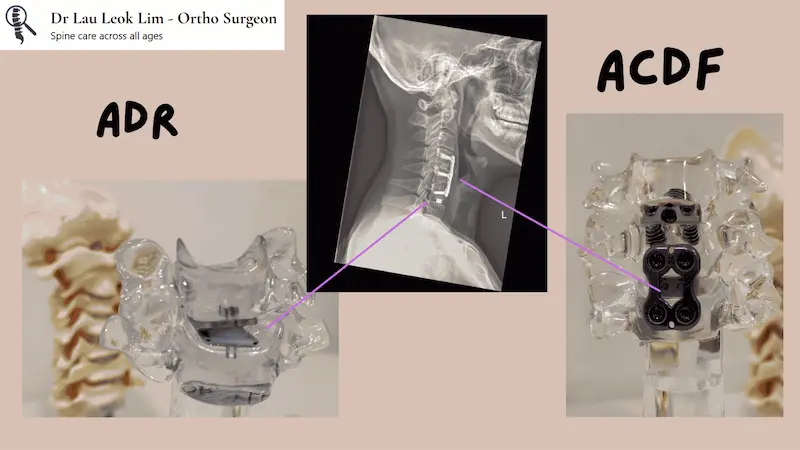
Fusion vs motion preservation: key differences between ACDF and ADR.
How Do We Choose Between ACDF and ADR?
| Factor | ACDF | ADR |
|---|---|---|
| Motion preservation | No | Yes |
| Best for | Severe degeneration, multi‑level disease, instability | Younger patients, soft disc herniation |
| Recovery | Similar | Similar |
| Long‑term risk | Adjacent segment stress & degeneration | May eventually turn into fusion (e.g., ACDF) |
| Suitability | Broad | More selective |
Recovery After ACDF or ADR
Immediately After Surgery
For single‑level surgery, most patients can go home the next day. For two or three levels, discharge timing is assessed individually.
First Few Weeks
Light activities are allowed. Avoid heavy lifting. A neck collar may be used depending on the procedure.
Long‑Term
ACDF requires time for fusion to occur. ADR preserves motion. Physiotherapy helps restore posture and strength.