Lower Back Pain Across Ages – Starting From the Basics
Why lower back pain happens, what structures are involved, and how patterns differ across age groups
By Dr Lau Leok Lim | lllau@orthohandpartners.com | Singapore | Published on 24 April 2026 | Last modified on 24 April 2026
Lower back pain is one of the most common reasons people seek medical attention. While many episodes are short‑lived, others reflect deeper structural, mechanical, or neurological processes. This page outlines the key symptoms, anatomical foundations, structural causes, and age‑specific patterns of lower back pain. For broader context on spine conditions across different life stages, visit the Children’s Spine, Teenagers’ Spine, Adults’ Spine, and Geriatric Spine.
1. Common symptoms of lower back discomfort
- Aching, stiffness, or tightness in the lower back
- Sharp or mechanical pain with bending or lifting
- Muscle spasms or tightness
- Reduced range of motion
- A sense of instability or “weak back”
- Clicking or catching sensations
- Pain radiating to buttocks or thighs
- Leg pain, numbness, or tingling
- Difficulty standing upright after sitting
- Morning stiffness that improves with movement
- Worsening pain with prolonged sitting
- Strong urge to stretch or self‑manipulate the back
2. Anatomy of the lumbar spine – the structural foundation
The lumbar spine is built to bear weight, absorb shock, and allow bending, twisting, and lifting. It consists of vertebrae, discs, joints, ligaments, muscles, and neural structures working together to support the upper body and protect the spinal cord and nerves.
Spinal alignment refers to how the vertebrae, discs, joints, and supporting soft tissues are stacked in a harmonious, energy‑efficient manner to maintain upright posture. When alignment is optimal, load is distributed evenly. When alignment is off, certain structures are overloaded, increasing the likelihood of pain, stiffness, and fatigue.
- Bones (L1–L5)
- Facet joints
- Intervertebral discs
- Ligaments
- Nerve roots and cauda equina
- Muscles and fascia
- Pelvis and sacroiliac joints
- Spinal alignment
3. What can go wrong – anatomical end‑points of pathology
fractures, spondylolisthesis, osteophytes
facet arthropathy, capsular injury, synovial cyst, sacroiliac joint dysfunction
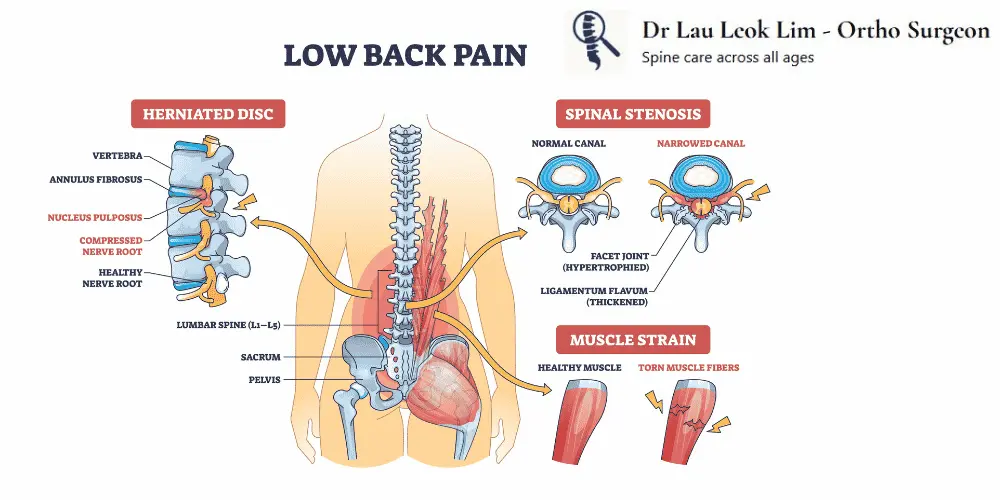
degeneration, bulge, herniation, annular tears, disc height loss, including patterns seen in degenerative disc disease, nerve root compression causing lumbar radiculopathy (sciatica), and canal narrowing contributing to lumbar stenosis.
sprain, capsular laxity, overstretching from sudden movements
strain, myofascial trigger points, postural fatigue
radiculopathy, neurogenic claudication, neuritis, including sciatica‑type symptoms from nerve root compression
loss of lumbar lordosis, pelvic tilt abnormalities, segmental malalignment, compensatory curvature changes
Hip pathology, sacroiliac joint inflammation, abdominal or pelvic organ issues, and even kidney‑related conditions may mimic lower back pain.
4. Pathological processes – why these problems occur
Some causes of lower back pain — such as tumours, infections, or fractures — may sound worrying, but these conditions are uncommon. Most people experience symptoms due to mechanical strain, inflammation, degeneration, or alignment‑related factors. Understanding the underlying process helps guide appropriate evaluation and treatment.
The body mounts an inflammatory response as the first step in repairing tissue injury. Increased blood flow and immune activity help initiate healing. However, excessive or prolonged inflammation can irritate surrounding tissues, causing stiffness, warmth, and pain.
Trauma may arise from sudden events — such as falls, twists, or heavy lifting — or from chronic repetitive strain, where repeated micro‑injury accumulates over time. Conditions such as sciatica may occur when trauma or disc injury irritates a nerve root. More details are available under slipped disc (lumbar disc herniation).
Degeneration is a gradual “wear‑and‑tear” process where discs lose hydration, joints stiffen, and cartilage thins. Bony spurs may form as the spine attempts to stabilise itself. These changes can alter load distribution and irritate nearby nerves.
Conditions such as rheumatoid arthritis or other inflammatory arthritides can affect the spine’s joints and supporting tissues. Autoimmune activity may cause stiffness, swelling, and pain, often worse in the morning or after rest.
Some individuals are born with structural variations — such as transitional vertebrae or mild spinal asymmetry — that may predispose them to mechanical strain or early degeneration.
Hormonal or metabolic conditions can weaken bone or soft tissue. A common example is osteoporosis, which increases the risk of vertebral compression fractures. More information is available under osteoporotic back pain in the elderly.
Spinal infections (discitis, osteomyelitis) or rare inflammatory conditions can cause persistent pain, fever, or night symptoms. These conditions are uncommon but require early recognition.
Abnormal spinal alignment can overload specific segments and alter muscle balance. Examples include leg length discrepancy, scoliosis, and degenerative disc disease, which can change spinal curvature and load distribution.
5. Lower back pain across ages – age‑specific considerations
Children
Lower back pain in children is unusual and should be evaluated carefully. When present, it may relate to sports overuse, stress fractures (spondylolysis), infections, or congenital abnormalities rather than typical mechanical strain.
Teenagers
Rapid growth spurts, changes in posture, and increased sports participation — especially in the context of immature bones — can predispose teenagers to lower back pain. Higher training loads may increase susceptibility to stress injuries such as pars fractures; more details are available under spondylolysis (pars fracture). Developing cartilage tissue is relatively weaker than bone, making adolescents more prone to apophyseal ring fractures than annular tears.
Adults
In adults, disc degeneration, facet wear, and muscle overload are common contributors. Lumbar radiculopathy (sciatica) may arise from disc herniation or foraminal narrowing. More details are available under spinal conditions in adults.
Older adults (geriatric)
Progressive degeneration, spinal stenosis, and reduced muscle mass may contribute to mobility‑limiting lower back pain. Neurogenic claudication — leg heaviness or fatigue when walking — is a common presentation. More information is available under spinal conditions in the elderly.